As the country braced for a second wave of COVID-19 cases, the rates at which Indian American and Alaskan Natives were being impacted became alarming.
In New Mexico, a state where this part of the population is only about 11% of the state total, they accounted for 21.50% of all COVID-19 cases by early November, according to data from the COVID Tracking Project.
The numbers become even more chilling when looking at the total number of deaths, as the percentage of Native American and Alaska Natives (AIAN) was almost half (44.66%). Even by national standards, that is notably high: the US average number of COVID-19 AIAN deaths per 100 people is 95, but that number jumps to 332 when looking at New Mexico alone.
“I feel like it’s almost criminal to let them die at such a high rate,” Jagdish Khubchandani, Professor of Public Health at New Mexico State University said.
Rate of COVIF-19 related AIAN Deaths per 100,000 people in different states. New Mexico has the secong highest rate (332) of the states that report this data, preceded only by Mississipi (682). Data from the COVID Tracking Project (13/12/2020).

Systemic issues that lead to poor healthcare and lack of access to basic services have put these communities at a disadvantage from the outset of the COVID-19 pandemic.
“Pandemics are not made in a day. Pandemics are made in decades. And preparedness is also not done in a day,” Khubchandani said. “[New Mexico] was a poor state before the pandemic, with such a diverse population that had chronically underfunded health systems. I think what we have is the sin of the past punishing us now. We have never prepared to deal with the pandemic nationwide.”
Abigail Echo-Hawk, M.A., Director of the Urban Indian Health Institute (UIHI) and chief research officer of Seattle Indian Health Board has been advocating for the importance of better systems of data collection about American Indian and Alaska Native communities.
“We have seen an underinvestment of public health systems and public health surveillance systems for many many years and we are seeing what happens when you don’t invest in public health,” Echo-Hawk said. “I feel like screaming about this for more than twenty years because we knew this kind of impact was happening in our communities, and for the very first time people are finally acknowledging it.”
The data for New Mexico seems alarming, but Echo-Hawk paints a graver picture. The actual amount of the AIAN population affected might be even higher because of racial misclassification, which results in the underreporting of race and ethnicity data for the AIAN population. A 2014 study by the CDS and Indian Health Service (IHS) found just that: there were “significant underestimates” of mortality estimates within the AIAN population.
“When you talk about the incredible amount of death that is showing on the current data trackers what we have to know is that is actually, in a very horrific way, a gross underreporting, because we know that death certificates are very often racially misclassified,” Echo-Hawk said. “There’s a very common saying for those of us that work in Indian country on data: that we are born native and we die white because we are racially misclassified on death certificates.”
This underrepresentation is a result in part of faulty racial classification systems in place in hospitals, according to Echo-Hawk.
“People instead of asking race and ethnicity will look at somebody who’s checking into a clinic, who’s come in for an appointment, being hospitalized or has died and decide what race or ethnicity they are without asking families and not asking the individual,” she said.
Across the US, many counties and states fall short of collecting all the health data necessary to keep track of how different communities are affected. In some cases, only a few options will be available for race — mixing all the rest together.
“The ‘other’ category effectively hides all other racial and ethnic groups,” Echo-Hawk said. “I call that a trash category. It is meaningless, it shows nothing and is an excuse for jurisdictions to say ‘well, we did our best’. That is effectively creating a category that hides the disparities of racial and ethnic groups.”
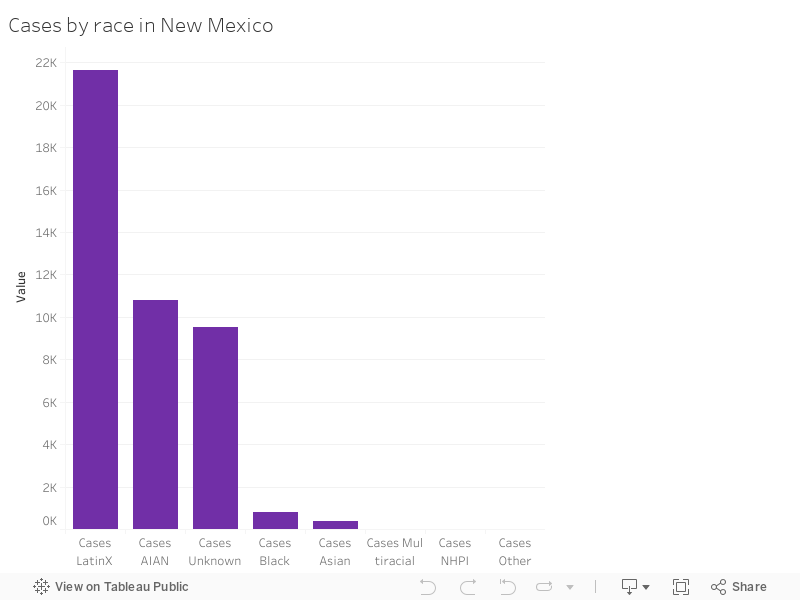
The chart below shows the total numbers of cases by race in New Mexico, in early November. About 21.50% were American Indian/ Alaskan Native. Data from the COVID Tracking Project (04/11/2020).
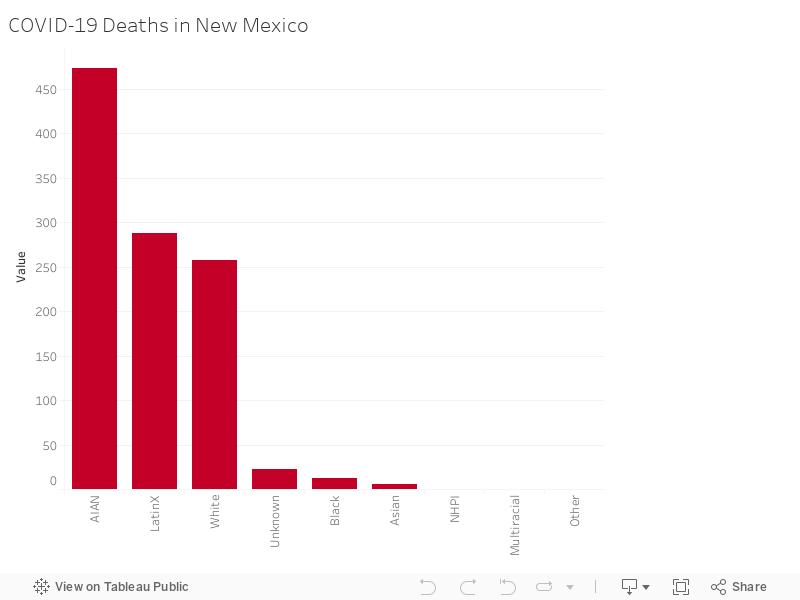
The chart below shows the total numbers of deaths by race in New Mexico, in early November. About 44.66% were American Indian/ Alaskan Native. The second most significat category is Latinx, followed by white. Data from the COVID Tracking Project (04/11/2020).
To understand the devastating effects of the pandemic on the AIAN population, Khubchandani says we have to look at both pre-causation factors and pandemic response issues.
“Much of what’s happening now with these populations and New Mexico is because of the historic underfunding and being historically marginalized,” Khubchandani said. “These are people who have very poor air quality. They don’t have water to wash their hands. They don’t have the resources and the money to buy materials, and they are getting sicker at a younger age, dying at a younger age than the national average. In part, because they have so many medical complications (…), which is related to poverty.”
Pamelya Herndon, 1st Vice-President of NAACP Albuquerque branch, pointed out one single issue as one of the most impactful in the spread of COVID-19 within AIAN populations.
“The biggest problem that we’ve seen with respect to the Native American population is there’s not enough running water,” Herndon said.
Data from the U.S. Census Bureau indicates that the average poverty rate in New Mexico for the past 12 months is 18.2% for the general population and 30% for 18.2%.
A 2018 Report by the New Mexico Department of Health found that when asked about their general health status white adults (16.6%) reported a significantly lower prevalence of fair or poor health than AIAN (24.8%). The same study indicated that AIAN adults had a significantly higher prevalence of obesity (42.8%) than all other races/ethnicities and that diagnosed diabetes was higher among AIAN (20.7%) than among White adults (9.6%).
These health socio-economic disparities felt by this population are co-related to the pandemic outcomes.
“These marginalized populations are more likely to not only contract Covid but to have extreme complications and to die,” Echo-Hawk said. “Health disparities are based on your socio-economic environment: Whether or not you have access to transportation, whether you have access to housing, whether or not there’s been gentrification in your neighborhood, whether or not you’re homeless.”
Access to healthcare is harder, not only because of geographic factors, for many who live in more remote areas, but also for cultural reasons. This means many of the COVID patients from AIAN communities who reach the hospital will already be in a more severe condition.
“Imagine if you have fever right now and you have to go 15 miles to see a doctor, most likely we’ll just let it go,” Khubchandani said. “Most of them seem to be living in areas where there’s no healthcare. It could be an urban neglected area or a tribal area where there’s no health care. And then it’s hard to reach out to the community. They have their own clanship and clan systems where they heal each other. Traditional medicine outreach has been weak.”
Communication is also a major issue, Khubchandani warned. While he believes New Mexico has fared somewhat good in this aspect, there is still a lot to be desired, especially when it comes to reaching out to people living in remote areas, who for example might not have a cellphone or speak English.
“The primary ways of communication on the Indian reservation is through radio,” Herndon pointed out.
Entities such as the Indian health service, which falls within the Department of Health and Human Services, play a crucial role in this outreach, but their jobs are hindered by the resources they lack.
“They have tried to do some word of the mouth, local flyers, and local info, but it’s not been aggressive enough,” Khubchandani said. “They have to be very aggressive. But that’s a difficult population to reach out to.”
Herndon said that there’s only so much the state can do in terms of requiring certain populations to follow their protocols.
“You have to remember that the reservations are independent nations, Herndon said. ”We do we really respect the fact that we have a nation within our own community that operates independently.”
Khubchandani believes that, while it’s one of the poorest states in the country, New Mexico’s overall response to the pandemic, on a larger scale has been exemplary when compared to other states — especially given that it’s working with very limited responses. The governor’s action has been stern, taking extreme measures when needed.
“I think New Mexico again is a role model, (…) given so many preexisting disadvantages, whereas I think there are places that had so much advantage and they messed up,” he said. “We have hard populations to reach out to. Navajo nations are not easy to deal with. But still, they did what they could.”