By: Maureen Mullarkey
Word Count: 1665
Lincoln County, Nevada – An Example of How the Second Wave Hits Rural Counties Across America, Straining Local Resources
Lincoln County, Nevada had only five cases of COVID-19 throughout the first seven months of the coronavirus pandemic. Zero deaths. With a population of 5,200 barely anyone in the county expected covid rates to soar beyond double digits. Then November arrived and Lincoln County held a testing positivity rate of 18.6%. Cases have since been skyrocketing, now totaling at 248.
“Two months ago it basically exploded,” said Lincoln County Sheriff Kerry Lee, 57. “It rapidly accelerated in the amount of cases.
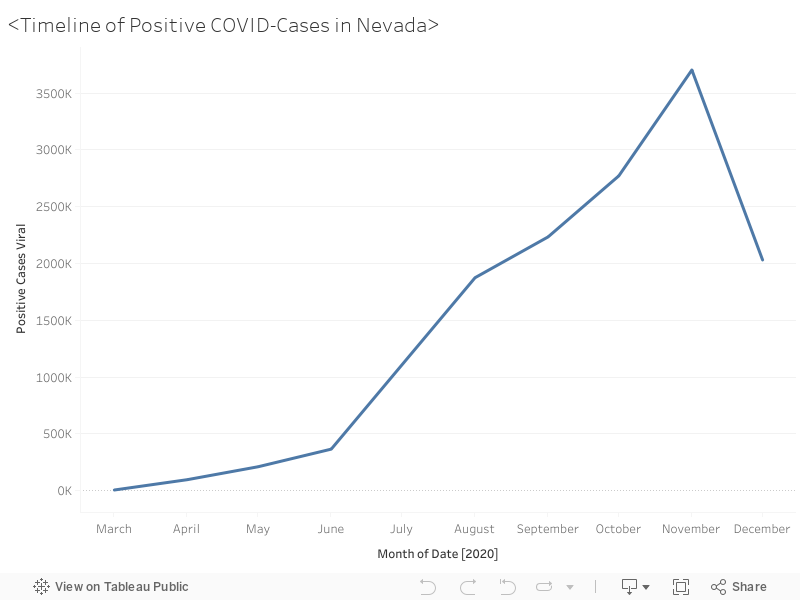
Lincoln County, one of Nevada’s most sparse and rural counties per square mile, now leads the state’s percentage of positive coronavirus cases, with a percentage of 62.7 percent at the beginning of this week. The county, which has a total population of 5,200, is just one of the many rural areas nationwide which are experiencing a surge of positive COVID-19 cases, in the second wave of the pandemic.
Shana Marie Loveday, a resident of the town of Alamo, has been a resident of Lincoln County since 1992.
“I don’t think people took it very seriously in the beginning,” said Loveday. “ You had to have your mask at the store, but you could shop without one until you got to the register. Some people didn’t even care if you had a mask. She said she herself didn’t worry too much, even when a healthcare provider she knew contracted the virus in the Spring.
“It was like, okay, that makes sense,” said Loveday, who works at a youth correctional facility. “You know, it was in a high risk field.
But come October, the county experienced its first COVID-19 related death, when an elderly woman in a nursing home contracted the virus. Then in late November, Lau Fiatoa, a healthy man in his 40’s, contracted the virus and died a few days later.
Loveday said Fiatoa’s wife was a former student of her husband, who teaches high school, and this affected the tight-knit community deeply.
“I feel like it was a big wake up call for a lot of people in the town,” said Loveday. “ It’s like, oh, so it took somebody dying, that’s kind of sad. You know, this poor man, he’s got four young boys at home. It just breaks my heart.”
Lee, who has been on the force for 32 years and sheriff for 16, said that this surge has not just affected the county’s residents but their resources as well. At the beginning of the pandemic in March, Lee says he tried to limit his officer’s interaction with residents to prevent exposure from COVID-19. But since most of his officers are also coroners for the county, and also serve as guards for the local prison in the town of Pinoche, limited exposure seemed almost impossible.
“We saw an increase in coroner cases not due to COVID, but an increase of fatal accidents. The traffic on our highways increased. Calls to service, [such as] domestics, calls contemplating suicide increase, everything that we do increased,” said Lee. “So we really had no choice but to go back. We couldn’t continue doing our job effectively with the precautions that we were taking. “
Lee’s department is made up of 16 officers, but as of now, four are in quarantine after exposure to COVID-19. Even though he felt his officers were given enough PPE this March, the lack of people power stretches his officers thin.
“Three or four doesn’t sound like a lot, but when you have a very small department, that’s big,” said Lee. “We’re requesting officers to work overtime. We shortened our shifts. We just basically did everything we could, and it’s still continuing right now.”
Lee says that even though his officers sometimes receive backup from other departments like Highway Patrol, there is no quick fix to replace a fully trained police officer. He says it takes almost a year for an officer to be trained and hired, especially in Lincoln County, where police wear multiple hats.
“In law enforcement, you just don’t hire somebody tomorrow and put them to work the next day,” said Lee. “ So hiring isn’t even an option for us as far as getting somebody to help fill the gaps.”
Lincoln County county, which is a total of 10,633.4 square miles, is mainly ranching county. North of Las Vegas, it only contains one hospital, Grover C. Dils Medical Center, which also is a nursing home.
Loveday says that while she feels this hospital is good for emergencies and has been transparent with the county about COVID-19 cases, residents often end up going to metropolitan areas for major health issues.
“I had an appendicitis years ago,” she said about one experience at Grover C. Dils. “And it was like, yep, ‘I think that’s what’s going on, get in, get over to Cedar City and get it taken care of there’.”
Dr. Bryce Putnam, the Health Officer for Elko County in the northeast of Nevada, says that one main issue rural counties face compared to metropolitan areas is a lack of infrastructure within its health care system. In Nevada, for example, its rural counties, or ‘frontier counties” are serviced by Carson City.”
“So just in perspective, it’s 320 miles from Elko to Carson City,” said Putnam. “We kind of had to work in conjunction with the state to use the existing resources that we had.”
Putnam says that in Elko county, in order to reach its almost 48,000 residents over 17,200 square miles, a COVID-19 Hotline was created in the first wave, where medical students from the University of Nevada answer caller’s questions about COVID-19. The medical students would be able to not only check someone’s symptoms over the phone, but create in-person appointments for them, if needed. The hotline encompassed six counties: Pershing; Humbodlt; Lander; Eureka; Elko; and White Pine.
Putnam says this hotline also relieved added stress from local sheriff’s offices and hospitals.
“They were able to stay home, not go into the doctor’s office, and, possibly propagate the disease, which is what we were trying to prevent,” he said.
Across the country, most non-metropolitan counties have now recorded at least 100 cases or more per 10,000 people since the pandemic began, more than double than in early September. Nevada as a whole has also seen an increase in almost every country, with an average of 2,429 cases per day. Elko County currently has 3373 total confirmed cases, and has experienced 28 COVID-19 related deaths
Putnam says that just because numbers are high in rural counties, it doesn’t mean there were not cases before in the first wave. With a lack of available tests, Putnam says medical students had to presume people positive for COVID-19 and tell them to stay home based on their symptoms, in order to keep the virus at bay.
“Back then, our biggest issue was that there wasn’t any testing. In rural Nevada, at one point we had 20 tests available for four or five counties,” said Putnam. “These things were like gold.”
According to the Salt Lake Tribune, Country Emergency Manager Eric Holt claims he was helping create a “recovery plan” to submit a state COVID-19 task force. Holt intends to increase testing and acquiring test kits which can be processed within 24 hours.
This increase of testing may be helpful, as Lincoln County’s percentage of positive cases has begun to decrease, starting with 62.7 percent on Monday, 52.7 percent on Friday, and 43 percent on Sunday. But still, Lincoln County has only administered 812 tests, according to the Nevada Health Response COVID-19 Statistics Dashboard.
Nevada governor Steve Sisolak had recently announced a three-week “pause” beginning on Nov. 24, putting heavier restrictions on businesses and stricter mask mandates. However, this mandate came after the 2020 presidential election, which may have been a possible factor in the increase of cases.
But Putnam says that these restrictions unfortunately fall at a time when people have a “pandemic fatigue”, when people are striving for some sort of normalcy in the pandemic, making it harder to expect others to comply with regulations. Putnam also attributes pandemic fatigue to the reason for a second wave, especially in areas like Lincoln County.
“When we were shut down, we were shut down for a long time,” he said. “That was absolutely detrimental to rural businesses.”
Loveday says that as essential workers, she and her husband’s work places have altered dramatically. As a youth correctional officer, she says the facility she works in, which normally houses 140 juveniles, has been cut in half to 56, lowering its yearly budget. She says her husband’s schedule as a high school teacher has also changed.
“In March, when they went in quarantine, our school district went online. He hated it,” she said. “Now he’s so excited to be back in the classroom. He’ll have a four day school week, and have classes that meet on Mondays, Wednesdays and another on Tuesdays and Thursdays.”
Loveday, who grew up in Las Vegas, said that most people who move to Lincoln County because they want a certain, more quiet lifestyle. A mother of two children ages nine and 17, the first wave was more tolerable for them because of fresh air.
“I let my kids do a lot more during the summer. They could go play out in the street,” she said. “They knew to keep your distance, but you can ride bikes and stuff with your friends. But now that it’s getting colder they don’t really want to be outside.”
City getaways were a bigger excursion, she says, and are now far away in terms of time as well as distance.
“As far as your day to day, most people just stay in your own little town. Each has a school and a church, a gas station and a market. But normally we’d go to Vegas and go to the movies for something fun. That would be fun to do again,” she said. “Someday.”