Tyson Foods attempts to mitigate PR nightmare while COVID-19 cases among Hispanic, Black, and Asian populations increase.
At the height of the first-wave of the COVID-19 pandemic, Hispanic, Black, and Asian front-line employees at meat-processing facilities worked shoulder-to-shoulder in low ventilated congregate spaces while taking orders from mostly white management who we now know wagered with their employes’ lives. The country experienced the height of the first COVID-19 wave of cases, fears, lockdowns, and anxieties with hot spots ravaging the country at long-term care facilities, meat-processing plants, and nursing homes. Now, eight months later in the midst of the deadly second wave, the US is making its way towards three-hundred thousand COVID-19 deaths and the meat-packing industry remains a national breeding ground for the virus. Throughout the past eight months, there have been some alarming allegations that led to lawsuits alongside global outrage of the country’s inability to keep the virus under control.
Tyson Foods, the global meat processing company which accounts for approximately twenty percent of the beef, pork and chicken produced in the United States, has been at the helm of these outbreaks. With a total of one-hundred and forty production facilities in the country, the majority of which are in Arkansas, Tyson has become an example of how being slow to adopt CDC recommended procedures and precautions can cost lives. The handling of the virus in these meat-processing facilities became so alarming, China suspended all poultry imports from Tyson Foods back in June, a major blow to the export business and brand reputation. Despite the public concern, Tyson Foods Senior Vice President Scott Brook shared in July, “we have more than 450 locations across the country, including some 140 production facilities, and a majority have not experienced any COVID-19 cases to date. In some of the sites where we have had cases of the virus, our prevalence is the same as the prevalence in the community. There are some sites where our numbers are higher than the community’s.” Brook and other senior management team members at the company have consistently applauded their internal efforts for implementing CDC recommended protocols, while also noting that community infections remain higher than company rates.
The below timeline offers a look into Tyson Food’s major COVID-19 updates alongside the rise in cases in Arkansas, beginning in April. [THIS WILL BE A TIME SERIES GRAPH THAT SHOWS THE RISE IN CASES ALONGSIDE THE ADDED MEASURES]
3/17/20: Tyson Foods issues first statement regarding intent to protect team members and ensure continuity of essential business. The company implemented employee travel restrictions, remote work and limited offices and facility visits. Updates to team policies include:
Relaxing attendance policies – eliminate punitive effect for missing work due to illness.
Waive 5 consecutive day waiting period for Short Term Disability benefits.
Waive the co-pay, co-insurance and deductible for doctor visits for COVID-19 testing as well as eliminating pre-approval or preauthorization steps.
Waive co-pays for the use of telemedicine.
Relax refill limits for 30 day prescriptions of maintenance medication.
3/31/20: Tyson Foods will pay approximately $60 million in “thank you” bonuses to 116,000 frontline workers and truckers in the U.S. who support the company’s operations every day to provide food during the COVID-19 pandemic. Eligible team members will receive a $500 bonus, payable during the first week of July.
4/17/20: Tyson Foods implemented new internal measures including taking worker temperatures, requiring protective face coverings, conducting additional cleaning and sanitizing and implementing social distancing measures such as installing workstation dividers and providing more breakroom space.
4/22/20: Tyson Foods temporarily closes its Logansport facility. Tyson Fresh Meats, the beef and pork subsidiary of Tyson Foods, Inc. indefinitely suspends operations at its Waterloo, Iowa, pork plant.
4/23/20: Tyson Foods temporarily closed its Pasco, Washington, beef facility.
4/27/20: Tyson Foods provides tour of plant facilities to a variety of state local healthcare and administrative professionals including:
Dr. Richard McMullen, state environmental health director and associate director for science, Center for Local Public Health, Arkansas Department of Health
Dr. Allison James, epidemic intelligence service officer with the CDC
Pansy James, RN and administrator, Dr. Bates Outreach Clinic, Arkansas Department of Health
Eldon J. Alik, consul general for the Marshall Islands Consulate General Office of Arkansas
A private primary care physician from Northwest Arkansas
4/29/20: Tyson Foods now offers $120 million in “thank you bonuses” for 116,000 U.S. frontline workers and truckers, up from the $60 million announced in early April. Tyson Fresh Meats, Inc., winds down production and will temporarily pause operations May 1 through May 4 at its Dakota City, Neb., beef facility to complete a deep cleaning of the entire plant.
4/30/20: Tyson Foods dispatched first mobile medical clinics will be on-site at facilities in Louisa County, Iowa; Waterloo, Iowa, and Logansport, Indiana. Additional medical clinics and mobile medical clinics will be deployed at Tyson facilities as needed.Tyson Foods partners with Matrix Medical Network to provide on-site healthcare including:
Diagnostic (PCR) testing of team members for COVID-19
Daily on-site clinical screening support at Tyson facilities to help ensure a safe working environment
Assistance with the environmental design of Tyson facilities to mitigate the risk of COVID-19 spread
Team member access to nurse practitioner care with access onsite or through a mobile health clinic
Employee education and support for personal health goals or concerns
5/1/20: Tyson Foods resumes operations in Logansport, Ind.
5/5/20: Tyson Fresh Meats resumes operations in Pasco, Wash. and Waterloo, Iowa.
6/1/20: Tyson Foods conducts facility-wide testing for COVID-19 at processing facilities and other operations in Benton and Washington Counties, where positive cases of the coronavirus have risen.
7/30/20: Tyson Foods has created a chief medical officer position and plans to add almost 200 nurses and administrative support personnel to supplement the more than 400 people currently part of the company’s health services team. The additional nurses will conduct the on-site testing and assist with case management, coordinating treatment for team members who contract the virus.
9/3/20: Tyson Foods is partnering with Marathon Health to pilot seven health clinics near company production facilities. The clinics will give Tyson team members and their families easier access to high-quality healthcare and, in most cases, at no cost. The stated goal is to promote a culture of health.
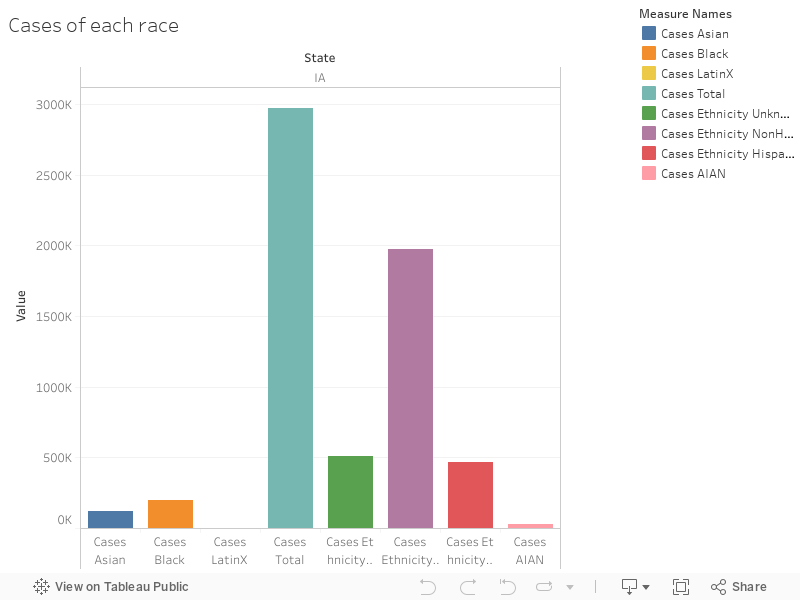
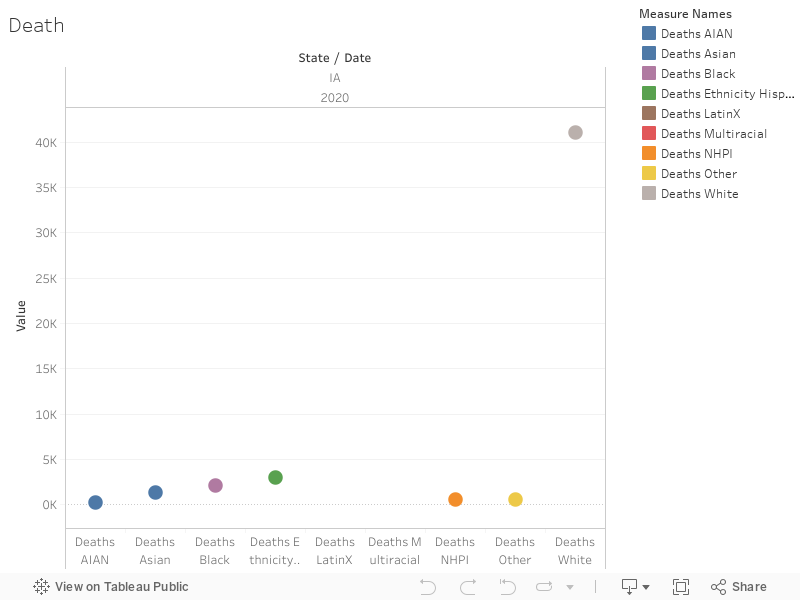
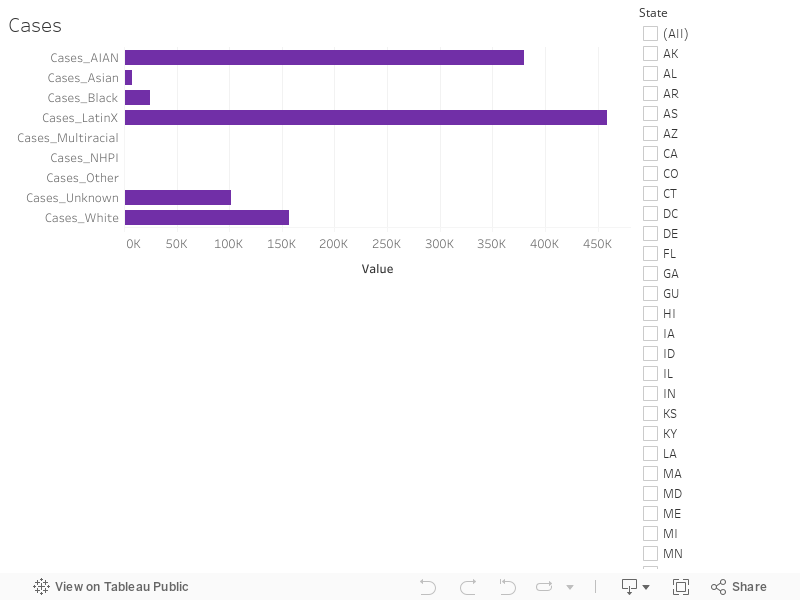
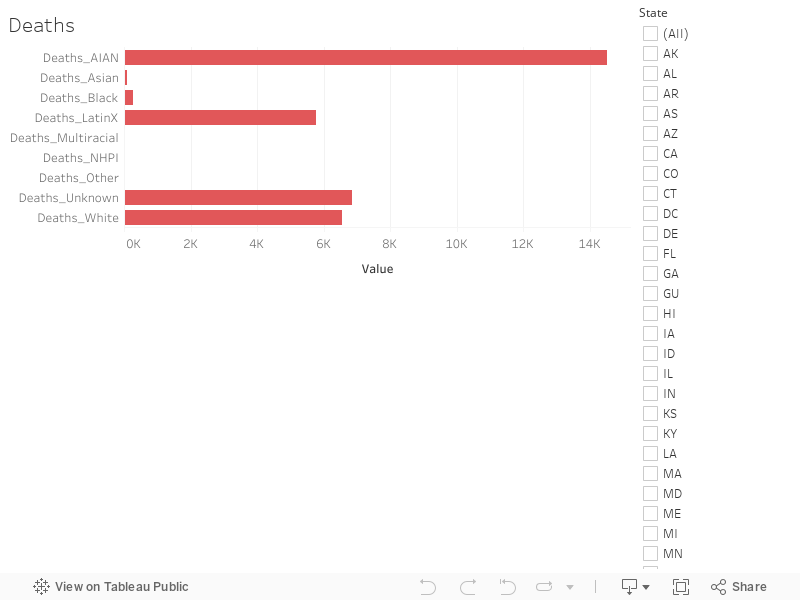
According to a new report from BuzzFeed News, these implemented policies come too late as seven meat processing plants in Arkansas owned by JBS, Tyson, and Cargill Tyson are accused of underreporting COVID-19 cases while the virus still has a stronghold on the workers. Congregate working conditions at these meat processing sites require employees to stand shoulder-to-shoulder in low ventilated warehouses with oftentimes unfavorable or non-existent paid-time-off policies. These conditions are having a disproportionate impact on the marginalized communities that make up the workforce at these processing plants. According to the CDC’s Morbidity and Mortality Weekly Report, “Among 23 states reporting COVID-19 outbreaks in meat and poultry processing facilities, 16,233 cases in 239 facilities occurred, including 86 (0.5%) COVID-19–related deaths. Among cases with race/ethnicity reported, 87% occurred among racial or ethnic minorities. Commonly implemented interventions included worker screening, source control measures (universal face coverings), engineering controls (physical barriers), and infection prevention measures (additional hand hygiene stations).”
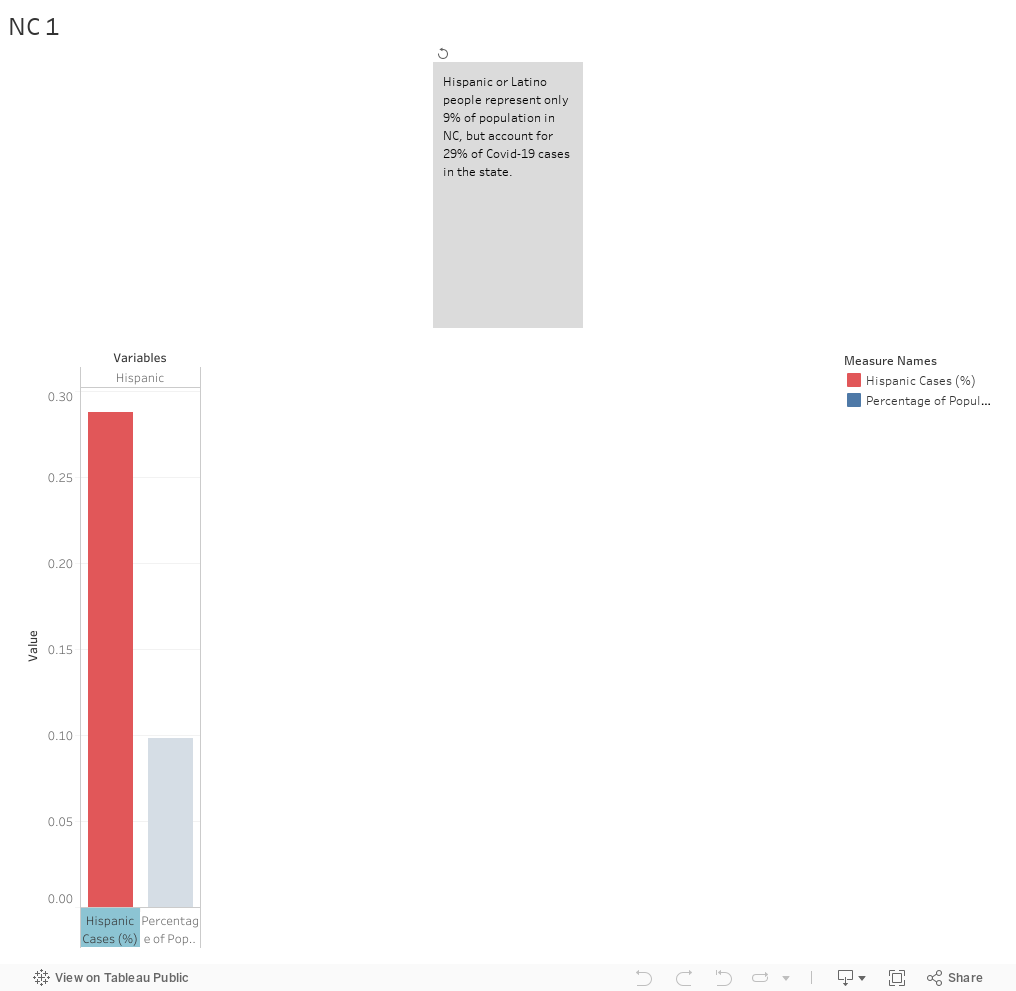
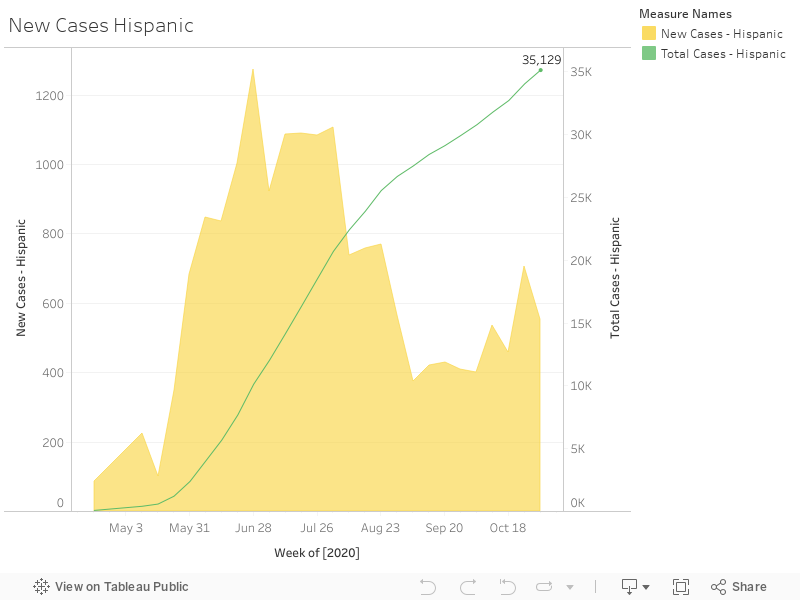
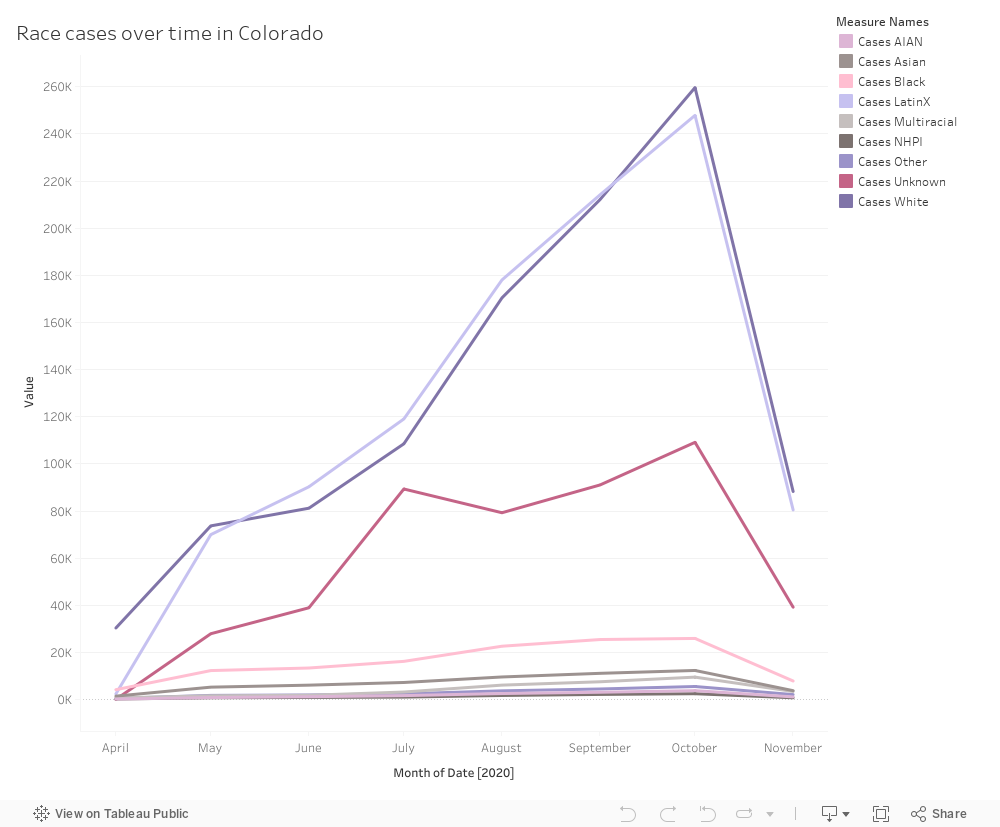
When looking at COVID-19 rates In the state of Arkansas, Hispanic/Latino residents make up 7% of the population, however make up 15% of confirmed COVID-19 cases. Springdale, AR —home to Tyson Foods Headquarters— happens to have the largest population of Hispanic/Latino residents (28,600), making up 36% of the city’s population of 76 thousand. The below graph highlights the rise in COVID-19 cases for Hispanic populations in Arkansas.
As seen above, the population’s COVID cases reached a staggering thirty-five thousand cases, making up 15% of total cases. Although new cases have leveled off, the second-wave continues to be of concern.
Aside from the poor publicity garnered from China cancelling its shipments, Tyson has a wrongful death lawsuit to atone for. According to CNN, Oscar Fernandez filed the wrongful death suit over the summer when his father Isidro Fernandez, an employee at Tyson’s Waterloo, Iowa plant, died from COVID-19 complications. The initial suit alleged Tyson did not take the proper precautions to ensure the safety of its employees. This month, the lawsuit was amended with allegations of malpractice and misconduct from Waterloo facility leadership. These allegations claim that management cancelled safety meetings, avoided the plant floors once COVID-19 cases were confirmed, encouraged employees to continue working regardless if they were sick or exhibiting symptoms, and most shockingly, management established “a cash buy-in, winner-take-all betting pool for supervisors and managers to wager how many employees would test positive for Covid-19.”
The official complainants include Food Chain Workers Alliance, Rural Community Workers Alliance, HEAL Food Alliance, American Friends Service Committee – Iowa, Idaho Organization of Resource Councils and Forward Latino. This Complaint alleges that the COVID-19 policies adopted after March 11, 2020 violate Title VI of the Civil Rights Act of 1964. This act protects individuals from racial discrimination by recipients of federal financial assistance. Complainants argue that “policies adopted by these companies cause a disparate impact on Black, Latino, and Asian workers and represent a pattern or practice of racial discrimination. The adopted internal policies reject common-sense protective measures, including a six-foot minimum of social distancing among workers critical to mitigate the risk of exposure to COVID-19. The internal policies discriminate on the basis of race by causing a substantial adverse effect on Black, Latino, and Asian workers. In addition, publicly available facts indicate a pattern or practice of discrimination. Existing social inequities compound this discrimination for Black and Latino workers, including higher death rates and higher hospitalization rates than white people.”