Lack of Information Contributes to Disproportionate COVID-19 Rates Among Oregon Latino Population
“It’s just really overwhelming,” said Anakaren Gutierrez Sandoval, a community health worker with the non-profit group Oregon Latino Health Coalition. “That’s the best way I can describe it. Everyone is just at max capacity.”
Sandoval is talking about the disproportionate affect that the COVID-19 pandemic has had on the Latino community in Oregon. While they make up about 12% of the population of Oregon, Latino Oregonians account for over 39% of coronavirus infections in the state. Several factors contribute to this – such as crowded housing, an overrepresentation of Latinos as essential workers, and lack of access to healthcare – but a leading consideration is the lack of information available to the community. While information on social distancing and mask-wearing seems to abound for English-speakers, resources in Spanish can be scarce.
“We have a 211 number where they could call to request assistance,” said Sandoval, “but a lot of times that was in English or they had technical difficulties being able to get that information.” Not only are Spanish-language resources hard to come by, misinformation on Spanish-language radio stations is plentiful. This lack of communication appears to have exacerbated or at least contributed to the disproportionate infection of the Latino community in Oregon.
“We’re in the middle of a pandemic,” said Mexican-American winemaker Cristina Gonzales, “But we’re also in a pandemic of misinformation. And that goes down the pipeline, down to our most disadvantaged and underrepresented groups.”
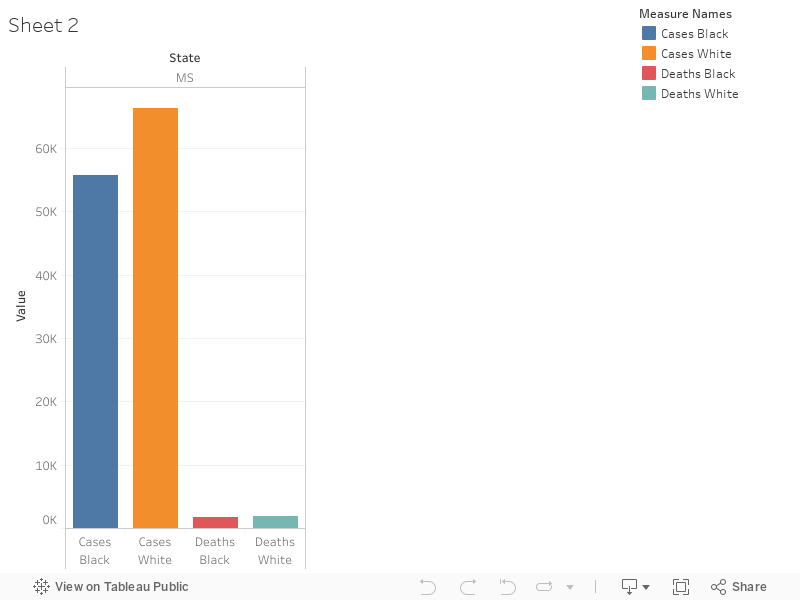
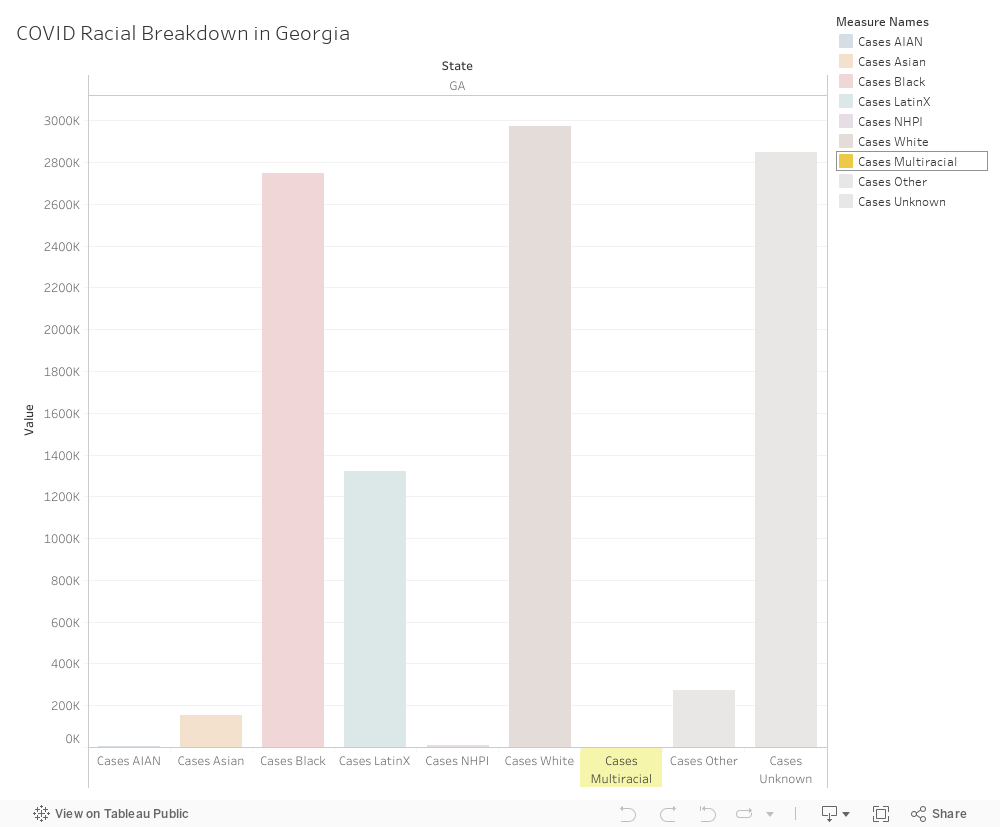
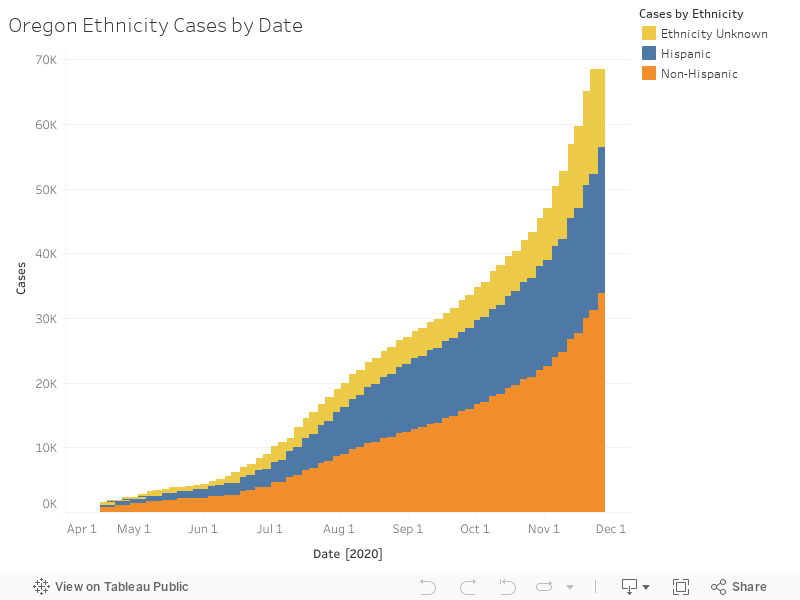
In the below graph, the blue bars represent positive tests of people who marked their ethnicity as Hispanic. While it is clear that these represent much more than 12% of the population, the data has been obscured in some ways by the differentiation between race and ethnicity.
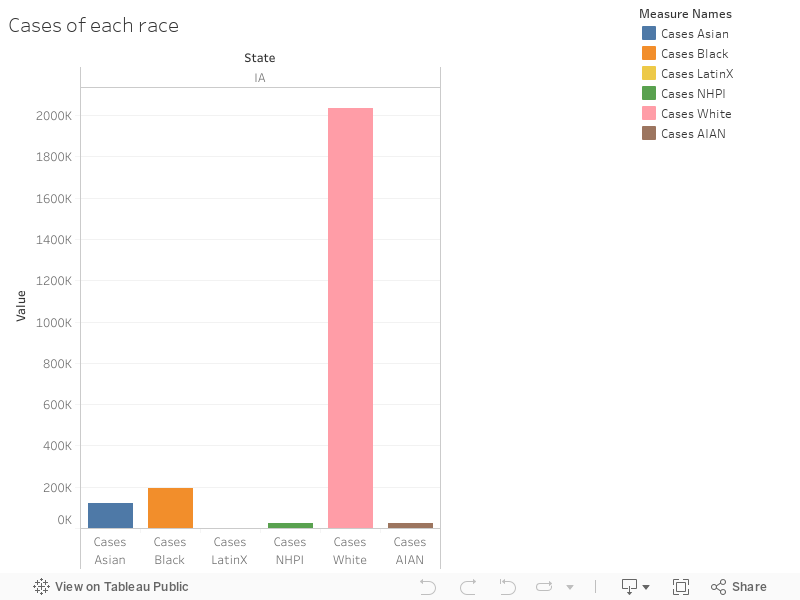
In this second graph, the “LatinX” community appears to have suffered zero cases – this is because most people mark “white” (or another race) as their race, and identify themselves using the Hispanic ethnicity box. This data could lead to an inaccurate analysis of the pandemic’s effect on the Latino community in Oregon.

This data shows the reality that Oregon’s Latino community, especially in the agricultural sector, has suffered disproportionately from the COVID-19. Most of Oregon’s agricultural workers – especially in industries such as the wineries and Christmas tree farming in the Willamette Valley – are Latino, many of them migrant workers. Since low-income housing can be hard to find, families crowd into small apartments, sometimes with two or three families in one two-bedroom apartment in the Portland area. This makes social distancing near impossible. For agricultural workers, losing two weeks of pay can be disastrous financially, and many employers aren’t doing enough to allow workers to take enough time off, or even let them know if those opportunities exist.
But working from home is impossible for agricultural and service workers, who make up a majority of the Latino population. For those who are students or who do work in other fields, at-home work can also be inaccessible due to a lack of reliable access to the internet. This dearth of technology, as well as the language barrier, mean that reliable news media is scarce. Many families rely on word of mouth, news from their home countries, (which can include misinformation or health advice that differs significantly from US standards), and accurate signage and resources at the place of employment.
And employers aren’t always equipped properly to meet the needs of the community. Gonzales, whose vineyard is located just outside of Portland in the Willamette Valley, said even when employers are well-intentioned, overwhelm and the financial stresses of the pandemic can affect how resources are distributed. “You see the public health care signs of, you know, let’s be safe during COVID,” she said, “And they have them that are bilingual and in different languages. But some of it is that the employers themselves might not know how to get it. Or it’s just not being posted to where workers are able to see it. And then there’s illiteracy, where workers are potentially not able to read if it’s in English or if it’s in Spanish.”
Another problem is trust. Even when translated into Spanish and made available, many Latino people may be wary of official sources. “There’s a lot of mistrust of the government,” said Dr. Roberto Orellana, a professor in the School of Community Health at Portland State University. “No matter if it’s local government or federal government, for a lot of people, government is government. And when the government put your kids in cages, you don’t trust the government.”
Orellana also underscored the importance of word-of-mouth and messages from community organizations, such as Latino churches or family members, to help get the right information across. “The message has to come from the government,” he said, “but also from … local organizations.”
Gonzales, in addition to being very active in the Latino wine-making community, is on the board of the non-profit AHIVOY, (Asociación Hispana de la Industria del Vino en Oregon y Comunidad). AHIVOY provides education to vineyard workers (called “vineyard stewards”) in order to help them overcome socioeconomic barriers and access other careers within the wine industry, such as sales, working in tasting rooms, marketing, and even becoming winemakers themselves. Through partnerships with local community colleges, AHIVOY has helped vineyard stewards, who might have started out as migrant workers, gain an immersive English-language experience as well as knowledge and resources to start fulfilling careers. However, Gonzales said the pandemic has put a halt to all of that. When the community college closed their campus and moved classes online in the spring, AHIVOY had to temporarily cancel its program.
“Vineyard stewards don’t have access to the internet all the time,” said Gonzales, “So that would make if very difficult to run classes.” In-person resources are a necessary part of catering to lower-income students. Gonzales said she hoped the program would be revamped in 2021, with smaller class sizes.
Shutting down schools or moving to remote learning has been a challenge for the Latino community, both for children who may not have access to the internet for online classes, and for parents who rely on the information pipeline passed through their often English-speaking children. Orellana emphasized that it is vital for schools to “continue to provide evidence-based information to the students so they can take it into the family.”
Sandoval said this information blackout has meant that getting the help her organization offers to Latino workers has been difficult. The Oregon Latino Health Coalition aims to help the Hispanic community in Multnomah County, especially those in the agricultural industries surrounding Portland, access otherwise hard-to-reach resources. They provide Spanish-language help with filling out applications for aid and healthcare. But Sandoval said that even in 2020, when much of life seems to have moved online, the group relies most heavily on word of mouth to get information to their clients. For a recent drive-through COVID testing event, Sandoval said, “Most of the patients that signed up for it, it was through word of mouth. When we would try to do it on social media, it wasn’t effective.”
Without adequate resources and information available to the Latino community, Sandoval also said that migrant workers fear giving the necessary personal information for contact tracing to county and state officials. They are afraid it might be given to ICE and lead to deportation.
“We saw a lot of clients hesitant to accept any sort of financial aid or resources, because they felt like it could affect their immigration status,” she said. Even though the county does not report any of the information it collects to ICE, Sandoval said people are hesitant to trust officials, and don’t want to disclose information such as the other members of their household. This has led to hesitance in the community to get tested, as a positive test is associated with having to disclose this vital information to the authorities.
Many involved in community outreach in the Latino community said that because resources and staff are scarce, it has led to extreme overwhelm among those trying to help. “Everyone is like a deer in the headlights right now,” said Gonzales. “We’ve been in the pandemic for a little while, but still, it’s so much to take in and process. And, you know, to try to survive.”
Because so much of Oregon’s Spanish-speaking population is currently employed in the agricultural and service sectors, there are too few Latino nurses, community health workers, and Spanish-speaking government employees to address the crisis. “When the vaccine comes,” said Orellana, “we want to have this large workforce of trained Latinos, who are bicultural and bilingual, that can help our agencies, the state and community health centers.”
Sandoval echoed the call. “We’re all feeling like there just need to be more resources available,” she said. “Because until people can feel like they can stay home, and take care of themselves, protect themselves, without losing their jobs or their homes, the numbers are still going to continue to increase.”