Iowa’s Asian Community Experience Increasing Racism Under COVID-19 Pandemic
By Shiyu Xu
During the pandemic, the Asian community has confronted the dual-threat: the infection of the Covid-19 virus and the infliction of xenophobic assaults.
In one of the whitest states in the country, the Asian community in Iowa has become more vulnerable to the increasing racial tension under the ongoing pandemic.
Shu Wan, a graduate student from the University of Iowa, launched a project called “An Oral History of Iowa’s Chinese Americans and Nationals Experiences during the COVID-19 Pandemic”, which conducts oral history research in three major towns in Iowa, including Ames, Iowa City, and Des Moines.
Through the research, many Asian individuals shared their experiences during the ongoing pandemic.
Rachel Li, a sophomore majoring in medical anthropology and music, has faced racism incidents while being on the University of Iowa campus.
When the U.S. began reporting its first COVID-19 cases in February, Li attended a comedy event hosted at the Iowa Memorial Union where an individual in the audience stood up and made a COVID-19 joke towards Asian Americans.
“I was one of maybe three Asians there,” Li said. “The host called him out, and I ended up approaching him to stand up for myself. He ended up leaving after he was confronted by both me and the host.”
During this fall semester, Li was walking on the UI campus surrounded by white students, when a maskless woman put her hand up to her face when she approached Li and immediately dropped it as soon as she passed her.
Caitlyn Valencia, a Filipino third-year and first-generation student, says she is frustrated with the racist language used to describe the virus.
“I don’t feel welcome here, and it’s not right because America is supposed to be built off of diversity,” Valencia said. “It’s sad that now privilege includes being looked at as a person instead of a scapegoat. Nowadays being Asian also means being viewed as a target for blame.”
Iowans of Asian or Pacific Islander descent make up 2.7 percent and 0.1 percent of Iowa’s population, according to the State Data Center, with Des Moines, Ames and Iowa City having the largest numbers. That percentage is projected to grow to 4.4% by 2050.
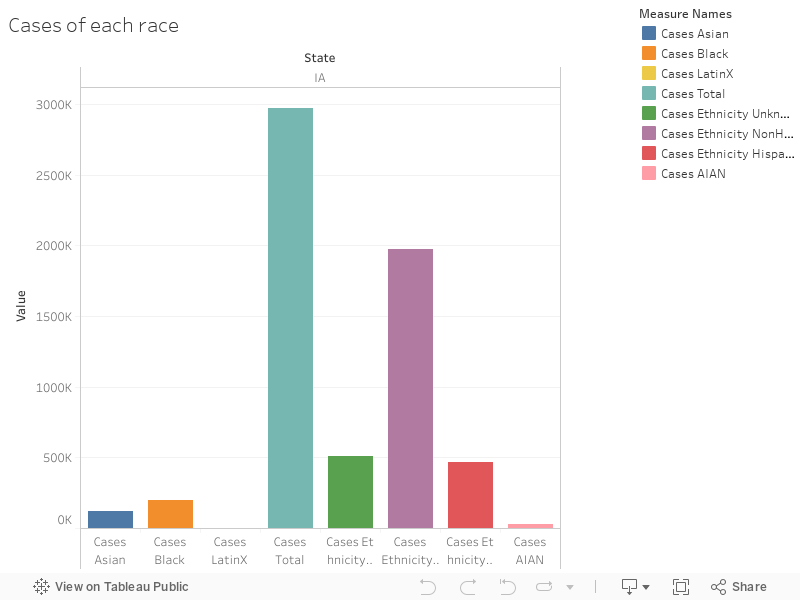
(The chart below shows the total positive cases among each race in Iowa. Among the minority races, Asian’s number is very close to the number for those who identify as black.)
(Although Asians only account for less than 3% of the Iowa population, they are suffering as much as the other racial minority groups.)
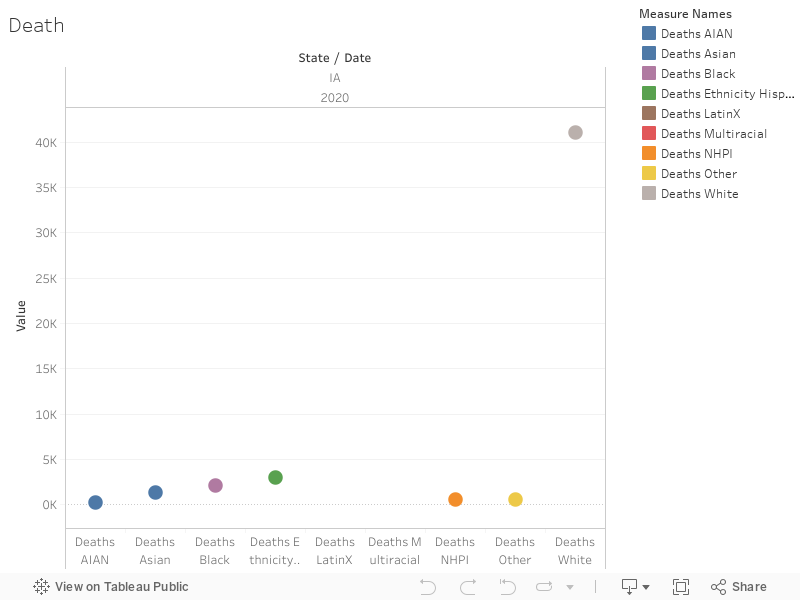
(The graph down below shows the number of deaths from Covid-19 among each racial group in Iowa. Similar to the total case number, the death number for Asians in the state is very close to the black and hispanic community.)
(With its population being less than 3% in the state, the death rate for Asian community is about 1.4%.) According to Iowa state’s Covid-19 data, more than 223,500 people have tested positive as of November 29. Among them, around 4,392 are Asian. The death rate for the Asian community in the state is 1.4%.
The Iowa Civil Rights Commission has received two race discrimination complaints filed by Asians so far this year, said Elizabeth Johnson, executive director of the commission. There were eight in 2019 and 12 in 2018. Eleven were filed in 2017 with eight in 2016.
Johnson said that under the Iowa Civil Rights Act, any person has 300 days from the last discriminatory incident to file a complaint alleging discrimination. “Therefore, it is entirely possible that many claims alleging discrimination related to COVID-19 have not yet been filed.”
To keep track of incidents in Iowa, the Asian alliance has created an online form where community members can submit reports of harassment and discrimination.
When Matuor Alier first started experiencing symptoms of COVID-19 in mid-October, he quickly took steps to isolate himself from his community in Fargo, a city on North Dakota’s eastern border with Minnesota. Alier, a 32-year-old social worker, quarantined in his home while enduring chills and fits of coughing; his wife experienced dizziness and headaches, and both of them grew concerned when their three-month-old child caught the virus, too.
“That was the scary part,” Alier said in an interview a month later, after he and his family had recovered. “The way that he breathed and the way that he coughed the entire night, when his body was aching.”
Alier, who came to North Dakota in 2008 as a refugee from what is now South Sudan, says he benefited from having a job that allowed him to work from home while he was ill. But the family was also able to receive help from a coalition of local nonprofit organizations dedicated to one purpose: helping North Dakota’s growing population of refugees and immigrants, particularly from Africa, survive the pandemic.
According to the latest data from the COVID Tracking Project, Black North Dakotans had the highest rate of COVID-19 cases relative to their population in the state, eclipsing even other vulnerable groups including Native Americans. While the state does not release racial data for deaths from COVID-19, the infection rate is over 9,000 per 100,000 for Black people, compared to about 7,200 for people identifying as white.
The virus has devastated African immigrant communities in the state, according to activists and government officials, as the state overall has endured a wave of infections in the fall, and currently has the highest case rate in the nation. In response, groups like the ESHARA Project — which stands for Ethnic Self Help Alliance for Refugee Assistance, and brings together seven community-based nonprofit organizations in the Fargo area — have stepped up to provide groceries, safe spaces to quarantine and translation assistance for non-English speakers seeking information about COVID-19.
“They don’t speak the language, they don’t have anybody advocating for them,” said Clarissa C. Van Eps, president of the North Dakota chapter of the National Association for the Advancement of Colored People, or NAACP. “We’re telling them that they have a safe space with us and telling them the things that we can do for them if needed.”
Nationwide, people of color have been disproportionately affected by COVID-19 due to a range of factors, including poverty, essential worker status and pre-existing health conditions. But the racial disparity in COVID-19 infections in North Dakota reflects larger trends particular to the state, which has experienced rapid demographic change in recent years. Over the past decade, the population of North Dakotans identifying as a race other than white has grown from just under 10 percent to 13 percent. The largest growth has been in the Black community, whose numbers have more than tripled since 2010, according to data from the U.S. Census Bureau.
The majority of this increase is driven by growing numbers of “New Americans” — a catch-all term for immigrants and refugees who have come to North Dakota seeking economic opportunity or political asylum. The percentage of foreign-born North Dakotans stood at 4.7 percent in 2018, up from just under 2 percent in 2000. While the state has significant populations of Asian immigrants, including Bhutanese refugees, the largest group identifies as Black, and includes immigrants from Somalia, Sudan, Liberia, Eritrea and the Democratic Republic of the Congo.
With a population of about 125,000, Fargo is North Dakota’s largest and most diverse city, and reflects many of these recent demographic trends. The city’s plentiful jobs in the manufacturing and healthcare industries, along with a relatively low cost of living, have attracted waves of immigrants, while North Dakota as a whole leads the country in refugee resettlement per capita.
But some of the very opportunities that pull New Americans to the region also make them more vulnerable to COVID-19, according to Hukun Dabar, executive director of the Afro-American Development Association of Fargo-Moorhead, which is part of ESHARA. Immigrants working manufacturing or retail jobs cannot work from home, while those in the healthcare industry spend more time in COVID-19 hotspots such as nursing homes and hospitals. Immigrant communities tend to be lower-income and less likely to own their own homes, while the state of North Dakota did not enact a rent moratorium during the pandemic.
“At the end of the month, the landlord wants the rent,” Dabar said. “They can’t stay home even one day from work, because they have kids to feed, they have rent to pay, they have bills to pay.”
Cultural and social factors heightened their vulnerability. Stigma against immigrants — who were sometimes blamed for spreading COVID-19, Dabar said — led some to avoid reporting their symptoms, while language barriers caused a general lack of information about the virus and its effects. Many immigrant families also live in large, multi-generational households where one infected person can spread the virus to multiple others, Dabar added.
Alier helped found ESHARA in 2016 as an employment assistance program for New Americans, and helped pivot the coalition to COVID-19 response in June. Throughout June and July, ESHARA coalition members helped nearly 300 people with rental assistance, grocery delivery services, and help getting tested for COVID-19 or filing for unemployment benefits.
Other groups have also stepped in to help, including the North Dakota chapter of the NAACP. The chapter, which was only created a few months ago in the wake of nationwide protests over racial justice and is still in the process of joining the national NAACP organization, has mustered volunteers and funds to distribute groceries and provide places to quarantine, according to Faith Shields-Dixon, the group’s vice president.
But it’s been difficult to see the disease ravage immigrant communities across the state, she noted.
“We’ve seen some loss of life — some of the pillars of the community have passed away from COVID,” Shields-Dixon said. “Everywhere people are dying from this disease. But we know that being able to provide those extra resources can lift the load off of them, and be able to assist them during this tragic time for them.”
Death data by race is unavailable in the state because the number of deaths among people of color is so small that releasing it would potentially allow individuals to be identified, a violation of health privacy regulations, said Grace Njau, an epidemiologist at the North Dakota Department of Health. But she said that despite the high rate of COVID-19 cases among New Americans, the rate of deaths for this population tends to be low because they are often younger and healthier than other groups.
At the same time, Njau said steps taken by the state to combat the virus can benefit all who are impacted by it. On November 14, North Dakota Gov. Doug Burgum implemented a statewide mask mandate and announced new restrictions on social gatherings for the first time since the start of the pandemic, complementing requirements that already existed in larger cities like Fargo and Bismarck. Njau said she sees this as a positive sign, and that the rate of new infections has already begun to drop.
“For now, I’m a little bit more optimistic in terms of our outlook,” Njau said. “But how long it lasts depends on how long we can keep up our masking and social distancing. If things hold at a steady state of where we’re at currently, I would say we’re heading in the positive direction.”
But even if cases drop, challenges will remain for New American communities in particular. Dabar said the state needs to provide more assistance to small business owners — many of whom are immigrants — facing losses due to COVID-19, while Alier added that children of immigrants tend to struggle with distance learning because their parents may not be able to afford the technology or help them if they don’t speak English.
“New Americans are taxpayers, they go to work every day, and they’re not people who always depend on benefits,” Dabar said. “So they need to see them as neighbors. They’re a big part of the state of North Dakota, because they’re not going anywhere.”
Lack of Information Contributes to Disproportionate COVID-19 Rates Among Oregon Latino Population
“It’s just really overwhelming,” said Anakaren Gutierrez Sandoval, a community health worker with the non-profit group Oregon Latino Health Coalition. “That’s the best way I can describe it. Everyone is just at max capacity.”
Sandoval is talking about the disproportionate affect that the COVID-19 pandemic has had on Hispanic and Latino communities in Oregon. While these groups make up about 12% of the population of Oregon, they account for over 39% of coronavirus infections in the state. Several factors contribute to this – such as crowded housing, an overrepresentation of Latinos as essential workers, and lack of access to healthcare – but a leading consideration is the lack of information available to the Hispanic community. While information on social distancing and mask-wearing seems to abound for English-speakers, resources in Spanish can be scarce.
“We have a 211 number where they could call to request assistance,” said Sandoval, “but a lot of times that was in English or they had technical difficulties being able to get that information.” Not only are Spanish-language resources hard to come by, misinformation on Spanish-language radio stations is plentiful. This lack of communication appears to have exacerbated or at least contributed to the disproportionate infection of the Hispanic community in Oregon.
“We’re in the middle of a pandemic,” said Mexican-American winemaker Cristina Gonzales, “But we’re also in a pandemic of misinformation. And that goes down the pipeline, down to our most disadvantaged and underrepresented groups. [They’re] not getting information or the correct information at all.”
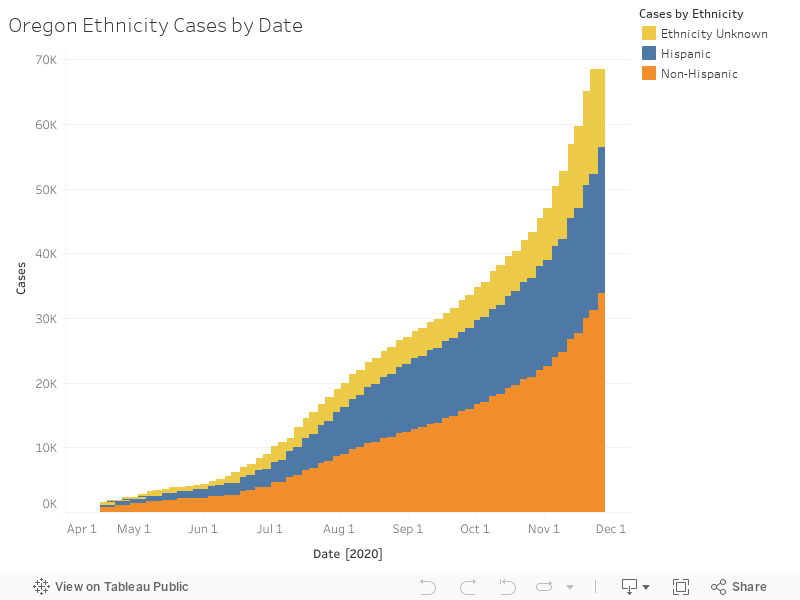
In the below graph, the blue bars represent positive tests of people who marked their ethnicity as Hispanic. While it is clear that these represent much more than 12% of the population, the data has been obscured in some ways by the differentiation between race and ethnicity.
In this second graph, the “LatinX” community appears to have suffered zero cases – this is because most people mark “white” (or another race) as their race, and identify themselves using the Hispanic ethnicity box. This data could lead to an inaccurate analysis of the pandemic’s affect on the Latino community in Oregon.
This data shows the reality that Oregon’s Hispanic community, especially in the agricultural sector, has suffered disproportionately from the COVID-19. Most of Oregon’s agricultural workers – especially in industries such as the wineries and Christmas tree farming in the Willamette Valley – are Latino, many of them migrant workers. Since low-income housing can be hard to find, families crowd into small apartments, sometimes with two or three families in one two-bedroom apartment in the Portland area. This makes social distancing near impossible, and without reliable access to the internet or accurate Spanish-language media, sometimes families don’t even know how they should be properly distancing and quarantining, even if they could. For agricultural workers, losing two weeks of pay can be disastrous financially, and many employers aren’t doing enough to allow workers to take enough time off, or even let them know if those opportunities exist.
Gonzales, whose vineyard, Gonzales Wine Company, is located just outside of Portland in the Willamette Valley, said sometimes even when employers and are well-intentioned, overwhelm and the financial stresses of the pandemic can affect how resources are distributed. “You see the public health care signs of, you know, let’s be safe during COVID,” she said, “And they have them that are bilingual and in different languages. But some of it is that the employers themselves might not know how to get it. Or it’s just not being posted to where workers are able to see it. And then there’s illiteracy, where workers are potentially not able to read if it’s in English or if it’s in Spanish.”
Gonzales, in addition to being very active in the Latino wine-making community, is on the board of the non-profit AHIVOY, (Asociación Hispana de la Industria del Vino en Oregon y Comunidad). AHIVOY provides education to vineyard workers (called “vineyard stewards”) in order to help them overcome socioeconomic barriers and access other careers within the wine industry, such as sales, working in tasting rooms, marketing, and even becoming winemakers themselves. Through partnerships with local community colleges, AHIVOY has helped vineyard stewards, who might have started out as migrant workers, gain an immersive English-language experience as well as knowledge and resources to start fulfilling careers. However, Gonzales said the pandemic has put a halt to all of that. When the community college closed their campus and moved classes online in the spring, AHIVOY had to temporarily cancel its program.
“Vineyard stewards don’t have access to the internet all the time,” said Gonzales, “So that would make if very difficult to run classes.” In-person resources are a necessary part of catering to lower-income students. Gonzales said she hoped the program would be revamped in 2021, with smaller class sizes. This is another example of how lack of internet access has harmed the Latino community’s ability to access resources that might help them navigate the pandemic, and even life after it.
Sandoval said this information blackout has meant that getting the help her organization offers to Latino workers has been difficult. The Oregon Latino Health Coalition aims to help the Hispanic community in Multnomah County, especially those in the agricultural industries surrounding Portland, access otherwise hard-to-reach resources. They provide Spanish-language help with filling out applications for aid and healthcare. But Sandoval said that even in 2020, when much of life seems to have moved online, the group relies most heavily on word of mouth to get information to their clients. For a recent drive-through COVID testing event, Sandoval said, “Most of the patients that signed up for it, it was through word of mouth. When we would try to do it on social media, it wasn’t effective.”
Without adequate resources and information available to the Latino community, Sandoval also said that migrant workers fear giving the necessary personal information for contact tracing to county and state officials. They are afraid it might be given to ICE and lead to deportation.
“We saw a lot of clients hesitant to accept any sort of financial aid or resources, because they felt like it could affect their immigration status,” she said. Even though the county does not report any of the information it collects to ICE, Sandoval said people are hesitant to trust officials, and don’t want to disclose information such as the other members of their household. This has led to hesitance in the community to get tested, as a positive test is associated with having to disclose this vital information to the authorities.
Both Sandoval and Gonzales said the situation has led to extreme overwhelm among those trying to help. “Everyone is like a deer in the headlights right now,” said Gonzales. “We’ve been in the pandemic for a little while, but still, it’s so much to take in and process. And, you know, to try to survive.”
“We’re all feeling like there just need to be more resources available,” said Sandoval. “Because until people can feel like they can stay home, and take care of themselves, protect themselves, without losing their jobs or their homes, the numbers are still going to continue to increase.”
During the Covid-19 pandemic, the South Sudanese immigrant community of Nebraska have been hit hard, trapped in poor working conditions in an uncertain economy. According to data from The Atlantic’s Covid Tracking Project, Black or African American Nebraskans account for 6% of Covid-19 deaths, though they only make up 5% of Nebraska’s population. As of November 18th, 2020, less than 1 in 10 Black or African American Nebraskans with Covid-19 sought hospitalization.
But what factors contribute to these troubling statistics?
Organizations like the Catholic Social Services of Nebraska, and the Lutheran Family Services of Nebraska help place South Sudanese immigrants in jobs throughout the state. According to Albert Maribaga, an elder in the community and employment specialist at the Catholic Social Services “it is hard to find jobs for South Sudanese immigrants, many do not come to America with formal educations and skills, and some cannot speak English”. As a result, South Sudanese community members often can only find work in meatpacking warehouses, nursing homes, and as housekeepers – all high-risk jobs in the Covid-19 pandemic.
Prior to, and through the pandemic, the Trump administration has pursued an aggressive deregulation agenda, reducing safety standards for industrial and service workers. In 2017, the Trump administration halted electronic reporting of workplace injury and illness reports by the Occupational Safety and Health Administration. In June 2018, Trump’s Center for Medicare and Medicaid Services halved fines for nursing homes that violated safe working condition practices. Although the federal government was pressured to require greater transparency from nursing homes regarding Covid-19 outbreaks in May 2020, nursing homes are not required to inform staff members about case rates in their facilities.
(should I put an interactive timeline here?)
But it is the conditions in meatpacking warehouses, such as the Smithfield Foods warehouse in Crete, Nebraska that have been the source of countless Covid-19 cases, and deaths. In February 2018, the Trump administration revised inspection standards for the Federal Food Safety and Inspection Service, reducing oversight of safety measures in meatpacking warehouses with the intent to increase food production. A recent federal lawsuit filed by the American Civil Liberties Union highlights the bleak working conditions of Nebraskan meatpacking plants, and how management’s unwillingness to adjust these conditions have created a breeding ground for infection. According to the ACLU, meatpacking workers “stand shoulder to shoulder for hours at a time on the processing lines, and they sit crowded together in a small windowless cafeteria where they cannot wear masks while eating”. “It’s a terrible cycle” said Maribaga, “young men go to work, get sick and don’t know it, and come home and infect their families”. To make matters worse, “if workers don’t get Covid in the factory, they get it while carpooling to and from the factory” said Christa Yoakum, Senior Welcoming Coordinator for Nebraska Appleseed’s Immigrants & Communities Program.
According to the Center for Disease Control, approximately 1 in 3 Black, non-Hispanic Nebraskans between the ages of 18-64 live without healthcare coverage. South Sudanese meatpacking workers have relied on their company healthcare plans to protect them and their families during the pandemic, all too often these healthcare plans are insufficient. “Infected workers are forced to stay at home without pay” says Maribaga “even if they want to seek care, they often cannot afford it because their budgets are so tight, or they haven’t worked long enough for their healthcare deductibles to kick in”. An unnamed source raised another issue with meatpacking healthcare; “sometimes the healthcare plans that these meatpacking workers receive are not accepted by local hospitals, and in-network hospitals are too inconvenient to get to”. According to Christa Yoakum, “even if workers had adequate healthcare, most Nebraskan hospitals are stretched thin and can longer provide acute care – this affects all Nebraskans regardless of race”.
The Nebraskan South Sudanese community faces socioeconomic factors, outside of poor working conditions, that contribute to the spread and fatalities of Covid-19. “Folks are scared to seek treatment because some are undocumented” says Yoakum “they have no social security numbers, so they couldn’t get treatment in most facilities even if they wanted to”. Christa Yoakum points out “often times both parents in a household get infected, because both work in the same facility. These households don’t have childcare resources adding extra stress to families while their breadwinners are sick on unpaid leave”. According to Cezar Garcia “often times meatpacking workers aren’t just providing for their immediate family, they support their extended family too” adding pressure for workers to continue working even if they are Covid positive. It is common in Nebraskan South Sudanese communities for older members to live with their families, because they cannot afford housing in assisted living centers. While younger family members with more robust immune systems can fight off the symptoms of Covid-19, elders perish. At the time of our interview, Albert Maribaga knew of five elders who had passed away that week.
Some Nebraskan institutions are developing programs to help their immigrant communities, centered around inclusion, employment, and awareness. For instance, in South Sioux City, newscasters have been broadcasting public service announcements about Covid-19 in the different languages of Nebraska’s immigrant communities. “These awareness initiatives are so important” says Cezar Garcia, a Community Organizer for Nebraska Appleseed’s Immigrants & Communities Program, “I have heard stories about people who don’t know when or how to wear their masks, and they’ve been relying on the news to get that information”. Food banks across Nebraska have adjusted their models for food delivery, opting to subsidize restaurants and grocery stores that serve foods from immigrant’s home countries. According to Christa Yoakum, an anonymous donor has financed an angel fund to help pay for the healthcare of Covid infected undocumented workers. The Worldwide Education Services have doubled down on their existing proposals to Nebraska’s state senate; lobbying for the certification of immigrant practitioners who held medical licenses in their home countries to be certified registered nurses and vaccine administrants.
The road to proper support for South Sudanese immigrants in Nebraska is long, but the Covid-19 pandemic has brought them unprecedented connection to non-for-profits. “Nebraska is a big state, we have relied on volunteers and word of mouth to build connections to immigrant communities” says Yoakum “now, we have direct communication with community members, and we will strengthen and deepen our ties with them to provide long term support”.
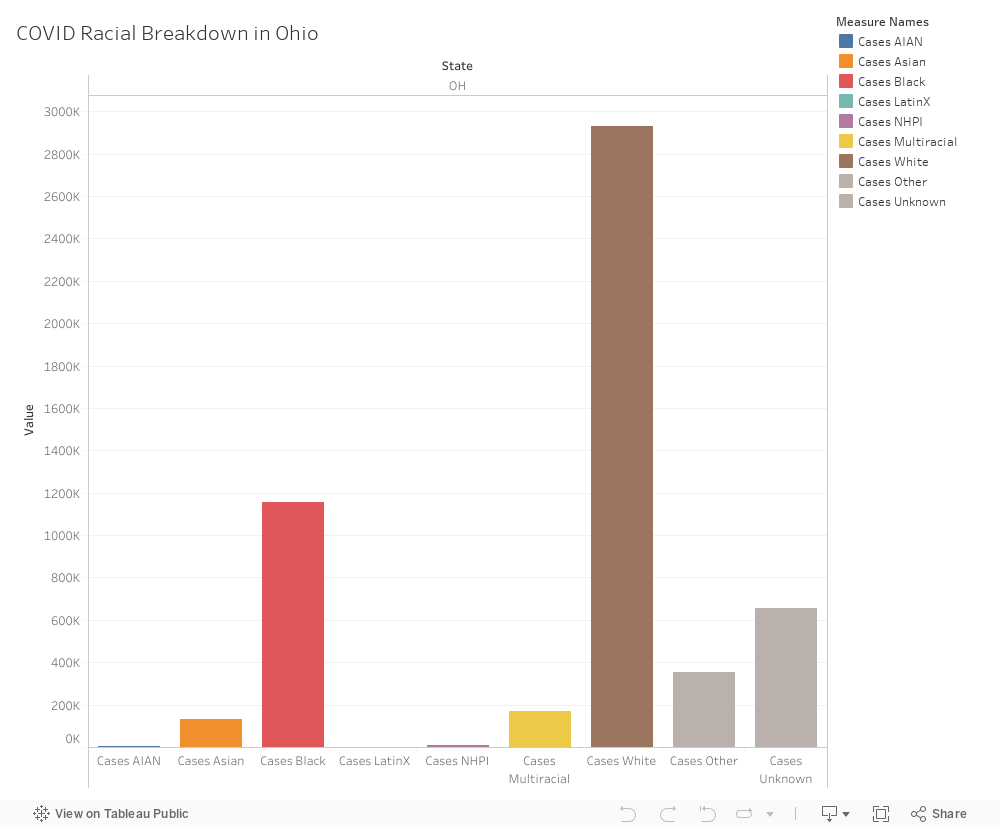
Though Black Ohioans make up only 14% of the state’s population, they make up 27% of COVID-19 hospitalizations and 18% of coronavirus cases in the state. The COVID Tracking Project flagged the group’s case proportion as suggestive of ethnic disparity due to three criteria: it is at least 33% higher than the Census Percentage of Population, it remains elevated whether the project includes or excludes cases with unknown race or ethnicity and it is based on at least 30 actual cases or deaths. It is no secret that the novel coronavirus has disproportionately affected Black, Native American and Latinx communities across the country.
Researchers from Ohio State University found that Black Ohioans have lower life expectancy and suffer from more chronic diseases than other groups. I propose a story focusing on the social and health factors that disproportionately affect Black Ohioans and contribute to the large proportion of COVID-19 cases in the state.
Potential sources:
Testimonies from Black residents who have tested positive for the novel coronavirus or families who have lost a loved one
Ohio Department of Health
Shawnita Sealy-Jefferson, a social epidemiologist at Ohio State University
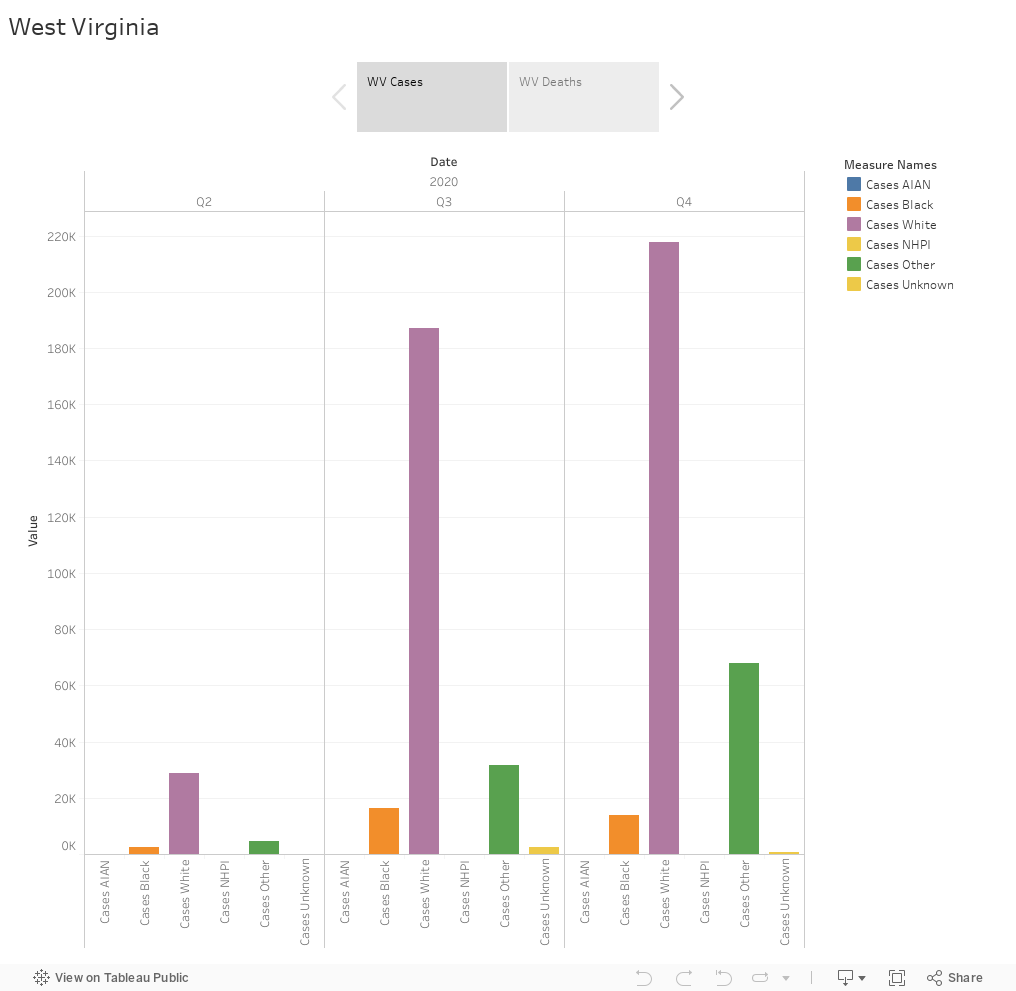
Pitch: One of the things that popped out to me while I looked at the data for West Virginia is how much of it is missing. West Virginia has been reporting COVID cases and deaths for races such as White, Black, Other, Multi-racial. They had reported on Native Hawaiians and American Indians/Alaskan Natives in between but stopped doing so. According do them, this is due to little or no data in those categories. Instead, they have grouped different races into one category called the “Other”.
According to the US Census Bureau, in 2019, WV had 93.1% White population, 3.7% Black, 0.2% American India/Alaskan Native, 0.8% Asian, 0% NHPI, 1.8% multi-racial and 2.4% other races. While the state itself seems to be predominantly white, discounting or aggregating races is an erasure of identity. I want to explore how doing this could have repercussions for the minority groups that are sidelined in the process. I also want to follow the data and see what options patients are given when reporting their race in hospital documents. I also want to ask West Virginia’s health department whether the decision to aggregate races was taken after consulting people from those races or not and why that decision was taken in the first place.
For this, I want to reach out to Abigail Echo-Hawk, director of Urban Indian Health Institute (UIHI) and the chief research officer for the Seattle Indian Health Board, who has been working for the data on indigenous community and fighting to correct racial misclassification. I recently came across her interview for science mag, where she said, “I see being eliminated in the data as an ongoing part of the continuing genocide of American Indians and Alaska Natives. If you eliminate us in the data, we no longer exist.”
For this I would like to talk to:
West Virginia Department of Health and Human Resources
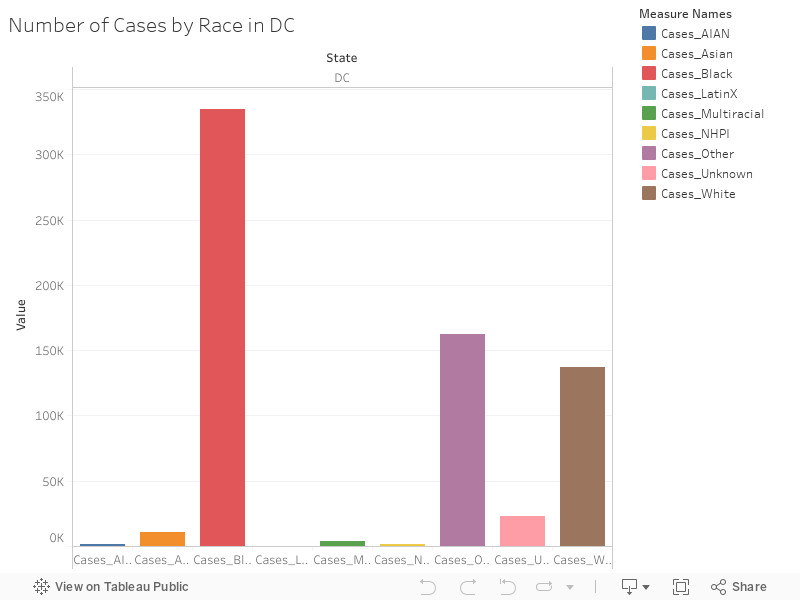
Acording to the US Census Bureau, white and Black/African American people both account for 46.0% of the population of DC. Yet, the COVID-19 cases data shows a completly different picture: cases among the Black population double the cases of the white population.
Upon some reaserch, I realized that the racial disparity between Black and white people in the District of Columbia, is the highest in the nation, according to ABC7.
A study published this week (Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis) looked into how patients from ethnic minority groups are disproportionately affected by COVID-19. It offers a few possible insights for this correlation:
“Individuals from ethnic minority backgrounds are more likely to live in larger household sizes comprised of multiple generations.”
“They are also more likely to have lower socioeconomic status, which may increase the likelihood of living in overcrowded households, or accommodation with shared facilities or communal areas
“individuals from ethnic minority backgrounds are more likely to be employed as essential workers, or less able to work from home, and as a result have continued to have contact with others through work or commuting.”
I would like to take into account these possible explanation factors and analizy how they apply to DC, in order to understand why the region of the US in specific has such a high disparity when it comes to the spread of COVID-19.
I would like to get in contact with epidemiology specialists who know this area well and with someone from DC Health, as well as organizations like the activist group DC Fiscal Policy Institute, which promotes opportunity and widespread prosperity for all residents of the District of Columbia, in order to piece all of this together.
“The clear evidence of increased risk of infection amongst ethnic minority groups is of urgent public health importance,” Dr. Shirley Sze, National Institute for Health Research (NIHR) academic clinical lecturer and a lead author of the paper told Business Insider.
Acording to the US Census Bureau, white and Black/African American people both account for 46.0% of the population of DC. Yet, the COVID-19 cases data shows a completly different picture: cases among the Black population double the cases of the white population. This might show a trend reproduced in other areas of the country, but I think it’s still interesting to look specifically at DC to understand the dynamics at play that result in a bigger impact of COVID-19 within the Black population.
Sources
DC Health
US Census Bureau
Debra Bernat, professor at the Department of Epidemiology and Biostatistics, at the The George Washington University
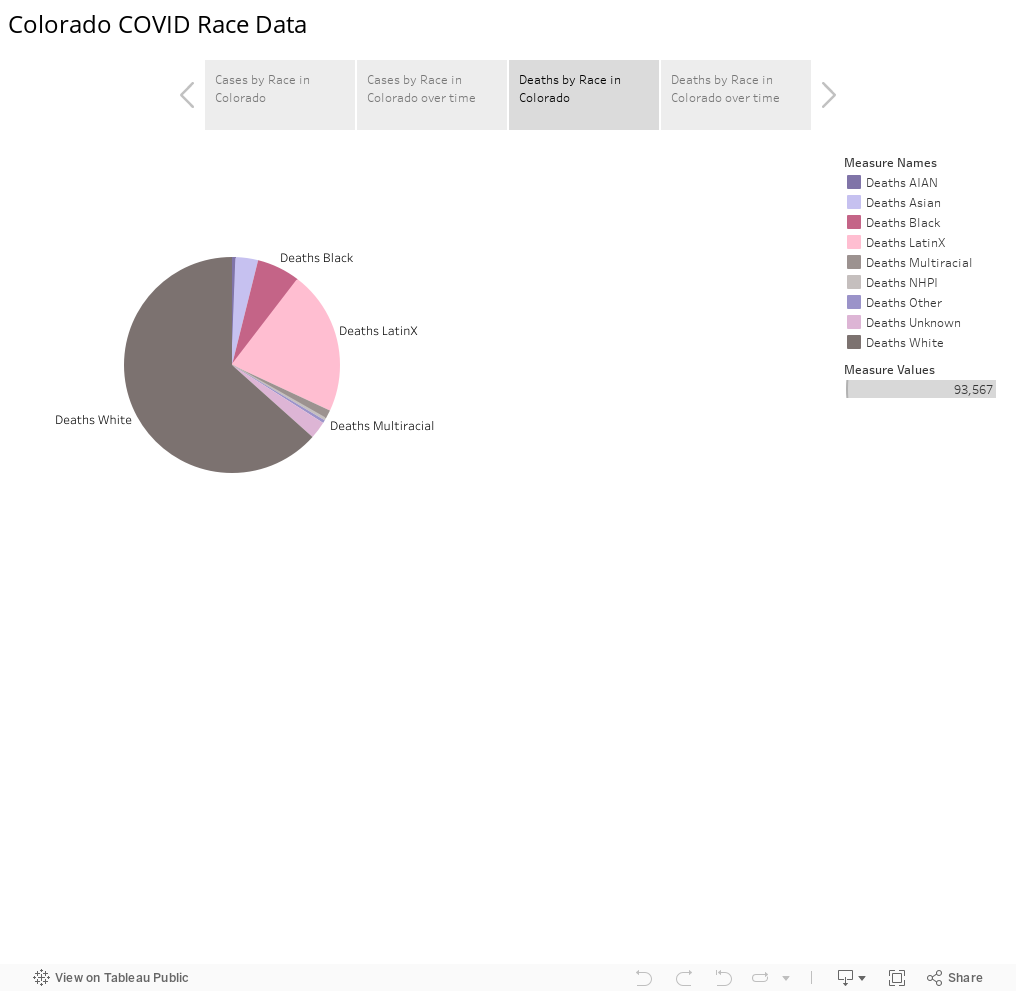
COVID 19 cases in Colorado seem to have disproportionately affected Latinx communities – especially when related back to the population per capita. Latinx people make up only 21% of the entire population in Colorado.
A possible reason that this is the case is that Latinx people tend to live in households with multiple people. Further, populations which usually have a lower median household income, or live in communities which may not have reliable access to healthcare, are also more likely to be affected by the coronavirus.
According to the Latino Leadership Institute, the median age of Latinos in Colorado is 27 compared to 42 for non-Hispanic whites, an age significantly younger and supposedly less susceptible to suffering serious COVID-19 consequences.
I would examine why COVID-19 has infected such a large amount of people in the Latinx community in Colorado, and examine how many cases translated into deaths, and how many people recovered.
I would also examine the age of the people who have died to see if it is mainly with an older population, or if a younger Latinx population is also being affected. I am curious about how the virus may have been transmitted – is it work-related or the larger families? – Would look at wage data and the total number of people in the household.